

An Overview of the Different Types of Diabetes Mellitus

Welcome to Morbus & Curis, a blog about disease and healthcare. Today’s blog post is about the different types of diabetes mellitus.
In my early twenties, I received a diabetes diagnosis that I’d never heard of. I was diagnosed with Maturity Onset Diabetes of the Young (MODY).
My MODY diagnosis made me wonder how many different types of diabetes exist and it turns out that there are many more than I expected.
Diabetes, or rather diabetes mellitus, is a term for a range of different diseases associated with high blood glucose levels. It includes the most prevalent types such as type 1, type 2 and gestational diabetes, as well as some other much rarer types.

This blog post will focus on the different types of diabetes mellitus. Diabetes insipidus is a separate condition caused by a deficiency of the hormone vasopressin, which results in the production of excess urine.
Type 1 Diabetes
Type 1 diabetes is an autoimmune disease that results in the destruction of pancreatic beta cells.
An individual’s immune system incorrectly identifies and attacks healthy pancreatic beta cells, which are responsible for producing the hormone insulin. Insulin is vital for instructing certain cell types to take up circulating glucose. As more and more beta cells are destroyed, insulin production and secretion falls. Eventually, the pancreas cannot produce sufficient insulin to regulate blood glucose levels and they rise.
The cause of type 1 diabetes hasn’t yet been determined, but it is believed that some people carry a genetic predisposition and certain environmental factors may impact a person’s likelihood of developing the disease.
Type 1 diabetes normally develops in childhood but it can develop at any age. It tends to develop faster in children than in adults.
As the disease progresses and blood glucose levels become uncontrolled, the following symptoms start to appear:

When a patient presents with diabetes symptoms, physicians most commonly use urine or blood glucose level tests to confirm a diabetes diagnosis. Since these tests only confirm whether the patient has hyperglycemia, further tests are necessary to determine which type of diabetes a patient has. Such tests include:
Ketone test
Glutamic Acid Decarboxylase (GAD) autoantibodies test
C-peptide test
The most common treatment for type 1 diabetics is regular insulin administration, to compensate for the lack or limited amount of insulin being produced by an individual’s remaining pancreatic beta cells. Insulin may be administered via a pump or by injection with an insulin pen.
Alongside insulin treatment patients are often educated on blood glucose testing and how it can be used to help them control their diabetes. They also receive education on how to balance their insulin doses to account for their level of physical activity and dietary carbohydrate intake.
While a healthy diet and maintaining a good level of physical activity is beneficial to all, in the case of type I diabetics it can help reduce the risk of longer-term diabetes complications. However, it cannot reverse their disease and type I diabetics must take insulin for the rest of their lives.
If a dose of insulin is too high or missed this can lead to certain short term complications. The most common ones include hypoglycaemia (when blood glucose levels become too low) and ketoacidosis (when blood glucose levels become too high).
The longer-term complications that may arise due to type 1 diabetes and poor management of blood glucose levels include:

Diabetes LADA
Latent Autoimmune Diabetes of Adulthood (LADA) is a form of type 1 diabetes that shares some of the characteristics of type 2 diabetes. It’s sometimes described as type 1.5 diabetes but that’s not an official term. A more accurate definition is “initially non-insulin requiring diabetes diagnosed in people aged 30-50 years old with antibodies to GAD.”
Whereas most cases of type 1 diabetes develop in children at a relatively fast rate (i.e. over days or a few weeks), LADA develops in adulthood and more slowly (i.e. over months or years). The slower disease progression is one of the characteristics it shares with type 2 diabetes and may sometimes result in a patient being mistakenly diagnosed with type 2 diabetes.
Early and accurate LADA diagnoses are important to ensure LADA patients are not inappropriately treated for type 2 diabetes. A LADA diagnosis is confirmed by the detection of elevated levels of pancreatic autoantibodies in diabetes patients who do not yet require insulin treatment. This is done via a GAD antibody test.
In addition to antibody testing, some clinical observations that may help health care professionals differentiate LADA from type 2 diabetes include:
Uncontrolled hyperglycaemia after treatment with common type 2 diabetes oral medicines.
Evidence of other autoimmune disease.
The patient does not have typical metabolic syndrome features such as a high BMI, high blood pressure and high cholesterol levels. However, someone with LADA can have metabolic syndrome features and this further complicates the diagnosis.
Many LADA patients do not immediately require insulin injections, but over time, as more beta cells are destroyed and less insulin is produced, treatment with insulin will be required. Similar to type 1 diabetes patients, LADA patients are also advised to regularly test their blood glucose levels.

Brittle Diabetes (Labile Diabetes)
Brittle diabetes is the term given to patients whose type 1 diabetes is very difficult to control and characterised by regular and extreme changes in blood glucose levels. Patients with brittle diabetes often experience severe episodes of hypoglycaemia or hyperglycaemia.
Although there is no obvious cause for the sharp change in blood glucose, potential causes include psychological issues, such as stress and depression, as well as nerve damage that affects the normal functioning of the digestive system.
For example, high levels of stress can result in periods of acute and temporary insulin resistance, which can make insulin dosing difficult. Dosing may also be made more challenging in patients with nerve damage to the intestines that affects how quickly glucose is absorbed into the bloodstream.
One treatment approach for patients experiencing brittle diabetes is to put them on a low carbohydrate diet. This can help minimise fluctuations in blood glucose following a meal, thereby reducing the frequency and severity of changes in blood glucose.
Given the challenges in determining insulin dosing, some brittle diabetes patients may use technologies such as insulin pumps, continuous glucose monitors or flash glucose monitors to better control their blood glucose.
Type 2 Diabetes
Type 2 diabetes occurs when certain tissues become resistant to insulin and the pancreas stops being able to make sufficient insulin to overcome this resistance, resulting in high blood glucose levels.
Initially, as insulin resistance develops, the pancreas produces additional insulin to overcome the resistance. So long as enough additional insulin is produced to compensate for the insulin resistance healthy blood glucose levels are maintained.
When insufficient insulin is produced to compensate for insulin resistance then glucose is not taken up into the cells of the body and remains circulating in the bloodstream, resulting in high blood glucose levels.
The most common symptoms of type 2 diabetes, which can develop slowly over months or years, include:

If a patient presents to a doctor with these symptoms then a fasting plasma glucose test or oral glucose tolerance test may be conducted to help diagnose type 2 diabetes.
There are several risk factors associated with a higher risk of developing type 2 diabetes, such as being overweight or a lack of physical activity. Other risk factors include:
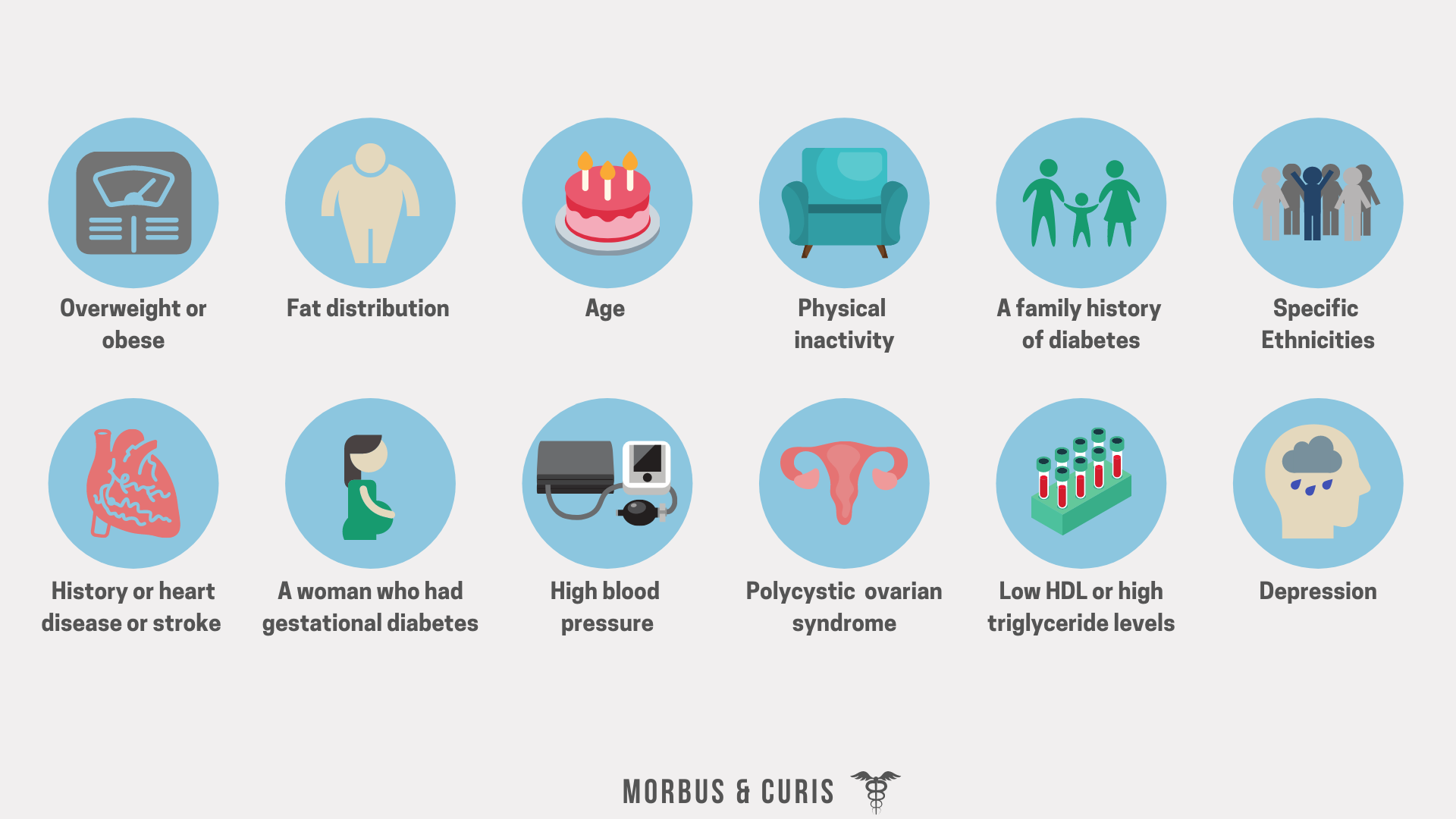
As many of the risk factors that can cause type 2 diabetes are associated with poor lifestyle choices, therefore the first-line treatment approach for many people with type 2 diabetes is to improve their eating and exercise habits. Some type 2 diabetics have been able to achieve a reversal of their disease progression or complete remission, through lifestyle improvement approaches.
If lifestyle changes are insufficient or ineffective at controlling a persons blood glucose (often defined as a HbA1c below 48 mmol/mol (6.5%)) the condition can progress resulting in patients requiring medication.
Medications available for the treatment of type 2 diabetes include:

High blood glucose levels can, over time, damage organs and lead to long term health complications. Long term health complications that may arise due to type 2 diabetes include:
Heart and circulatory disease (including stroke)
Neuropathy (nerve damage)
Retinopathy (eye disease)
Nephropathy (kidney disease)
Slow healing
Hearing impairment
Depression
Sexual dysfunction
Skin conditions
Sleep apnea
The impact of these complications can be huge, from reducing a person’s ability to work to increasing the amount of care they require from health care professionals and family. However, if a persons type 2 diabetes is well managed they can minimise the risk of developing these conditions.
Double Diabetes
Double diabetes occurs when a person with type 1 diabetes develops insulin resistance, a key characteristic of type 2 diabetes. This is more common in type 1 diabetes patients who are obese since that is the main risk factor for developing insulin resistance.
People with double diabetes fail to produce sufficient insulin and their cells fail to adequately respond to insulin.
Treatment management for patients with double diabetes can be challenging. They require higher doses of insulin but that can lead to weight gain. Additional adipose tissue can exacerbate insulin resistance and further increase a patient’s required insulin dose.
Gestational Diabetes
As the name suggests, gestational diabetes is a temporary form of diabetes that can develop while a woman is pregnant. It typically presents during the third trimester then disappears after childbirth. However, women diagnosed with gestational diabetes are at an increased risk of later developing type 2 diabetes.
The hormonal changes that occur during pregnancy increase insulin resistance. This requires an expectant mother to produce several times more insulin than normal to maintain normal blood glucose levels. If the higher insulin demand is not met, then blood glucose levels will rise and gestational diabetes is diagnosed.
Gestational diabetes is believed to affect somewhere between 1 in 7 and 1 in 20 pregnant women and risk factors that may increase a women’s chances of developing it include:

In the UK, gestational diabetes is normally tested for between 24 to 28 weeks gestation via the Oral Glucose Tolerance Test (OGTT).
Many pregnant women diagnosed with gestational diabetes can manage the condition by improving their diet and increasing their activity level, but some may require insulin treatment. Ensuring blood glucose levels are well managed during pregnancy is important to increase a woman’s chances of having a healthy child.
The aim is to keep blood glucose levels between 4-7 mmol/L and HbA1c within the normal non-diabetic range (less than 48 mmol/mol (6.5%)). If a pregnant women’s blood glucose levels are very high then her urine should be tested for ketones, because ketoacidosis, which occurs at very high blood glucose levels, can be fatal to the developing foetus.
Type 3 Diabetes
Some evidence suggests that Alzheimer’s disease should be classified as type 3 diabetes.
It was recently discovered that insulin resistance can occur in the brain during the progression of Alzheimer’s disease. When neurons in the brain are no longer able to respond to insulin, key functions of the brain, such as memory and learning, decline. However, Alzheimer’s disease is not characterised by hyperglycaemia in the brain.
Diabetes MODY
MODY stands for Maturity Onset Diabetes of the Young.
It’s the name given to a group of monogenic diabetes all caused by single point mutations in genes that affect pancreatic function. The term MODY was used because, in most subtypes, the condition normally develops before the person reaches the age of 25.
MODY is estimated to affect about 1-2% of people with diabetes. Inheritance is autosomal dominant, meaning the mutant variant of a gene is dominant and you only need one mutant copy to be affected by the condition. Accordingly, a carrier of a single mutant variant has a 50% chance of passing the mutated gene onto their offspring.
To date, 13 different subtypes of MODY diabetes have been discovered. Their prognosis and treatment vary. For example, some subtypes of MODY result in a patient having symptoms present from birth whereas others do not cause symptoms to appear until adolescence.
Neonatal Diabetes
Neonatal diabetes is a very rare, monogenic form of diabetes that is diagnosed under the age of six months old. There are two types; transient and permanent.
It’s caused by mutations to genes involved in insulin production. The mutations lower insulin production resulting in higher blood glucose levels, which are normally treated with insulin or glibenclamide.
Around a fifth of infants who have neonatal diabetes experience developmental delays, such as learning difficulties or muscle weakness.
Drug-Induced Diabetes
Drug-induced diabetes occurs when a medication raises blood glucose levels. This typically occurs when the medicine disrupts insulin signalling or causes damage to pancreatic beta cells, and the effect may be temporary or permanent. Examples of medicines that can induce diabetes include beta-blockers, thiazide diuretics, psychiatric drugs, anti-seizure drugs, niacin, HIV treatments, pentamidine and steroids.
Steroid-Induced Diabetes
Glucocorticoids are a class of corticosteroids that are often prescribed to reduce inflammation and treat diseases caused by an overactive immune system. However, when corticosteroids are given to people for a prolonged period of time (i.e. longer than 3 months) or to people who have a higher risk of developing type 2 diabetes, this can lead to steroid-induced diabetes.
This is because of the effect corticosteroids have on our blood glucose levels. By mimicking the stress hormone cortisol, corticosteroids increase our blood pressure and blood glucose levels, and this can lead to insulin resistance.
Steroid-induced diabetes can be temporary with blood glucose levels returning to normal after treatment. If blood glucose levels do not return to normal, because an individual has developed the 2 diabetes during steroid treatment, this is known as steroid-induced type 2 diabetes.
Secondary Diabetes
Secondary diabetes occurs when a separate medical condition results in high blood glucose levels, sometimes permanently, by various different means.
Conditions that can cause secondary diabetes, either through insulin resistance or by limiting the body’s ability to produce insulin, include:
Cystic fibrosis
Polycystic ovary syndrome (PCOS)
Pancreatic cancer
Hemochromatosis (an iron disorder)
Chronic pancreatitis (inflammation of the pancreas)
Cushing's syndrome (a condition where the body produces too much cortisol)
Glucagonoma (a condition where the body produces too much glucagon)
Pancreatectomy (surgical removal of the pancreas)
Acromegaly ( a hormonal disorder where the body produces too much growth hormone)
Hyperthyroidism (an overactive thyroid)
How secondary diabetes is managed depends on the condition that caused it.
For example, when a condition leads to insulin resistance (e.g. Cushing’s syndrome), lifestyle changes and/or oral therapies such as metformin are often used to help manage blood glucose levels.
If a condition causes secondary diabetes via a loss of pancreatic function and reduced insulin production (e.g. pancreatitis or cystic fibrosis) then insulin is the most common treatment approach.
Rare Genetic Disorders associated with Diabetes
Finally, some rare genetic disorders are associated with diabetes. These include:
Wolfram Syndrome is associated with childhood-onset insulin-dependent diabetes mellitus but unlike type 1 diabetes the cause is genetic, not autoimmune. It’s treated with insulin injections.
Alström Syndrome is associated with insulin resistance that develops in young adulthood, that often develops into type 2 diabetes.
Sources
https://www.nhs.uk/conditions/diabetes/
If you found this blog post helpful why not consider subscribing.