



Maturity-Onset Diabetes Of The Young

Welcome to Morbus & Curis, a blog about disease and healthcare. Today’s blog post is an overview of Maturity-Onset Diabetes Of The Young.

I wanted to write about Maturity-Onset Diabetes Of The Young (MODY), a group of different types of monogenic diabetes, for two main reasons:
I have one of them.
Awareness of MODY is not as widespread as it is for type 1 and 2 diabetes.
A Personal Experience
Before diving into the details, here’s my personal experience with introducing MODY.
When I tell people I have MODY I’m nearly always met with the same reaction; a mix of surprise, confusion and curiosity.
Often people have never heard of the condition. That’s not surprising since MODY is a rare condition that was only discovered in the last 30 years or so.
The majority of the time the response I receive from healthcare professionals is curiosity. I have, however, had awkward and challenging moments when explaining to healthcare professionals that I have MODY.
For example, during a new patient health check at my GP practice, a nurse tested my urine sample, then informed me that I didn’t have diabetes. At this point, I mentioned that I been diagnosed with a rare type of monogenic diabetes. She turned and looked at me aghast. Her expression read of one of disbelief. Fortunately for me, there was a medical student in the room whom, upon seeing the nurse’s face, interjected and explained that he had heard of MODY and it was, in fact, a real condition. I then briefly explained to the nurse which subtype of MODY I have.
Then came another awkward moment reminiscent of a Little Britain “the computer says no” sketch. The computer system only wanted to accept type 1 or type 2 diabetes diagnoses. In the end, the nurse had to choose one and write extra notes to clarify my real diabetes diagnosis.
If I found myself in a similar situation, I would direct the healthcare professional to the Diabetes Genes website and the University of Exeter MODY team.
What Is Maturity-Onset Diabetes Of The Young?
So what is MODY?
It’s the name given to a group of monogenic diabetes all caused by single point mutations in genes that affect pancreatic function. The term MODY was used because, in most subtypes, the condition normally develops before the person reaches the age of 25.
MODY is estimated to affect about 1-2% of people with diabetes. It runs in families and inheritance is autosomal dominant. This means that the mutant variant of a gene is dominant and you only need one mutant copy to be affected by the condition. Accordingly, a carrier of a single mutant variant has a 50% chance of passing the mutated gene onto their offspring. On the bright side, they also have a 50% chance of passing on their normal gene onto their offspring.

Subtypes of MODY
To date, 13 different subtypes of MODY diabetes have been discovered. Their prognosis and treatment vary. For example, some subtypes do not require therapeutic interventions whereas others do. Additionally, some subtypes of MODY result in a patient having symptoms present from birth whereas others do not cause symptoms to appear until adolescence.

Although many distinct subtypes of MODY diabetes have now been identified, the four most common subtypes of MODY diabetes are GCK, HNF1A, HNF4A and HNF1B. They have varying clinical courses and treatments.
GCK MODY is caused by a point mutation to the glucokinase enzyme of the pancreas whereas HNF1A, HNF4A, and HNF1B are caused by mutations to pancreatic transcription factors.
GCK MODY
GCK MODY accounts for approximately a fifth of UK MODY cases and is characterised by mild, sustained hyperglycaemia that is stable throughout life. The condition is caused by a mutation to the gene encoding the pancreas’s glucose-sensing enzyme, glucokinase. The mutation impairs the enzyme’s function and causes a right shift in its activity curve, resulting in glucose homeostasis occurring at a higher level (i.e. a fasting glucose measure between 5.5 and 8.0 mmol/l is normal for an individual with GCK MODY, whereas unaffected non-diabetic individuals have fasting glucose measures below 5.4 mmol/l).
Treatment
GCK MODY doesn’t require treatment and people with GCK MODY show a very limited glycemic response to blood glucose-lowering agents such as insulin. This is because their body counter regulates the effects of these therapeutic agents via the secretion of counter-regulatory hormones.
Pregnancy
GCK MODY can cause complications during pregnancy if the fetus does not inherit an affected mother’s GCK variant. This is because the mother will be exposing the fetus to mild, sustained hyperglycaemia. This increases the risk of fetal macrosomia (a large birth weight, >4 kg) and birth complications, such as shoulder dystopia. Previously some mothers were treated with insulin, but since this treatment has a limited ability to lower the mother’s blood glucose, it has a negligible effect on the birthweight of the offspring and is no longer recommended.
Fetal growth can be monitored via additional ultrasounds in the third trimester and if macrosomia is detected, then induction of labour around 38 weeks of gestation may be recommended.
HNF1A MODY
HNF1A MODY diabetes accounts for 50-60% of UK cases of all MODY diabetes. It occurs when a mutation in the HNF1A transcription factor gene progressively lowers the amount of insulin that is produced by the pancreas over the course of an affected indivivual’s life. If left untreated this can result in glycosuria (excess of sugar in the urine) and damage to the small blood vessels in the eyes and kidneys.
Treatment
People with HNF1A MODY are treated with sulphonylureas, which help increase the amount of insulin produced by the pancreas. However, these patients need to be treated with low-dose sulphonylureas as they exhibit enhanced sensitivity to sulphonylureas. If given the standard dose prescribed to patients with type 2 diabetes they can become severely hypoglycaemic.
As this type of MODY diabetes is progressive, patients may later require treatment with dipeptidyl peptidase-4 (DPP-4) inhibitors, glucagon-like peptide-1 (GLP-1) receptor agonists or insulin, in addition to low-dose sulphonylureas.
People with HNF1A MODY diabetes are also at increased risk of coronary heart disease, regardless of their HDL levels, thus it’s often recommended that they are also treated with cholesterol-lowering medications.
Pregnancy
While fetal inheritance of HNF1A mutant variants does not result in increased birth weight or incidence of hypoglycemia it may cause congenital hyperinsulinism. Furthermore, management of glycemic control with glyburide (a sulfonylurea), which can cross the placenta, may increase in the risk of macrosomia and neonatal hypoglycemia. Accordingly, pregnant women with HNF1A may be switched to insulin therapy during the second and third trimesters of their pregnancies.
HNF4A MODY
Similar to HNF1A, the HNF4A mutation also causes the amount of insulin produced by the pancreas to decrease over the affected individual’s lifetime. The symptoms of HNF4A MODY are also similar to those of HNF1A MODY.
Treatment
HNF4A MODY is also managed with sulphonylureas and, as it progresses, patients may later need to administer insulin in addition to low dose sulphonylureas.
Pregnancy
HNF4A-MODY pregnancy outcomes are dependent on the fetal genotype. If the fetus inherits the mutant variant there is an increased risk of fetal macrosomia. This risk is greatest when the HNF4A mutant variant is inherited from an affected mother vs. an affected father, because of the effect of maternal hyperglycemia.
There is also an increased risk of neonatal hypoglycaemia (low blood sugar), which can sometimes require treatment.
Accordingly, tight maternal glycemic control is important and current treatment approaches are similar to HNF1A MODY (mothers are switched to insulin treatment for their second and third trimesters). Additional ultrasounds are also recommended to assess fetal growth and if macrosomia is detected, then induction of labour or elective cesarean section may be considered before 38 weeks.
HNF1B MODY
The pathology of HNF1B MODY diabetes is quite distinct since the HNF1B transcription factor affects the HNF1B protein which is found in many organs and tissues (e.g. the kidneys, pancreas, reproductive tract and liver). Accordingly, a mutation in this gene results in a multisystem disorder.
The most common symptoms are renal manifestations, such as renal cysts. Kidney abnormalities due to HNF1B MODY are variable; some people are only mildly affected while others may experience kidney failure.
If renal manifestations and diabetes are both present then the condition is often referred to as Renal Cysts and Diabetes (RCAD). Most often diabetes develops in adolescence or young adulthood.
Other features of HNF1B MODY include a smaller-than-average-sized pancreas, pancreatic atrophy, gout, and uterine and genital tract anomalies. See here for a full list of clinical features.
Treatment
HNF1B MODY diabetes is usually managed by treatment with insulin and people with the condition show a limited response to other blood glucose altering agents.
Pregnancy
HNF1B MODY can cause abnormalities of the reproductive tract (e.g. differently shaped uterus) that can affect the ability to conceive or have a successful pregnancy.
MODY Diagnoses
Diagnosing MODY is challenging because there is a lack of distinct clinical criteria (e.g. age of onset, BMI, HbA1c levels) to identify potential MODY patients. This makes accurate diagnoses of MODY near impossible in the absence of genetic testing.
The most commonly used criteria to select potential MODY diabetes patient are:
Age of onset of before 25
A parent affected with diabetes
No previous insulin treatment
However, even these criteria can result in many cases of MODY diabetes going undetected or being misdiagnosed.
To improve MODY diagnoses a “MODY Probability Calculator” was developed, which uses complex modelling, statistics and an assessment of multiple criteria. The calculator requires details on multiple patient clinical features such as BMI and HbA1c, then determines a Positive Predictive Value (PPV) of the patient having MODY.
Once a potential MODY patient has been identified the diagnosis can be confirmed via genetic testing. Subsequently, appropriate treatment recommendations can be made, ensuring the patient doesn’t receive unnecessary or ineffective therapeutic interventions.

The calculator was developed by the diabetes team at the University of Exeter Medical School and can be accessed online or on their Diabetes Diagnostics app. Note that the calculator is more reliable at diagnosing MODY where a patient has not previously received insulin treatment.
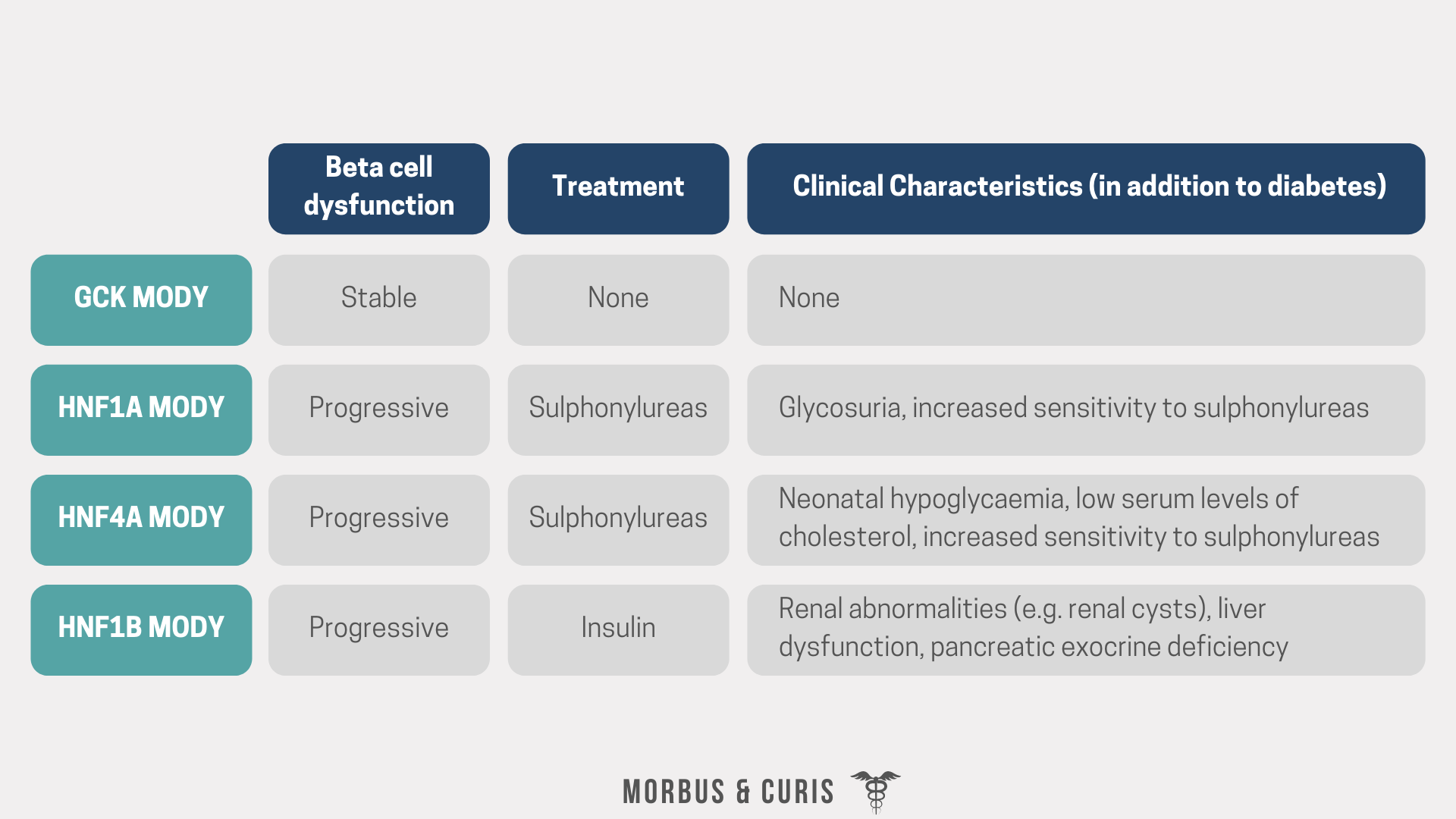
MODY Subtype Summary

Sources
Clinical Management of Women with Monogenic Diabetes During Pregnancy
The Netherlands Journal of Medicine - Maturity onset diabetes of the young: Seek and you will find
If you found this blog post helpful why not consider subscribing or sharing this post.
Cover photo credit: Matt Chesin on Unsplash