



Medicine Pricing in the UK

Welcome to Morbus & Curis, a blog about disease and healthcare. Today’s blog post is about the medicine pricing in the UK.

In the UK, medicines are freely priced by the manufacturer and, until recently, were not subject to price controls. Instead, the government historically relied upon market competition and voluntary agreements with the pharmaceutical industry to manage the cost of medicines.
However, in the last couple of years new legislation, as well as new provisions in the current voluntary scheme with the pharmaceutical industry, have granted the government some control over medicine pricing. The main objectives of these new provisions are to cap the annual growth of the NHS branded medicines bill and to prevent excessive prices being charged for unbranded generics.
The direct and indirect price controls that may be applied to a medicine depend on several factors such as whether the medicine is a brand or a generic, where in the product lifecycle the medicine is and whether the manufacturer is a member of the Voluntary Pricing and Access Scheme for Branded Medicines (VPAS).

Branded Medicines
Manufacturers are still able to freely set the list price of most branded medicines in the UK. However, the growth cap on total annual NHS spending on branded medicines is effectively an indirect price control.
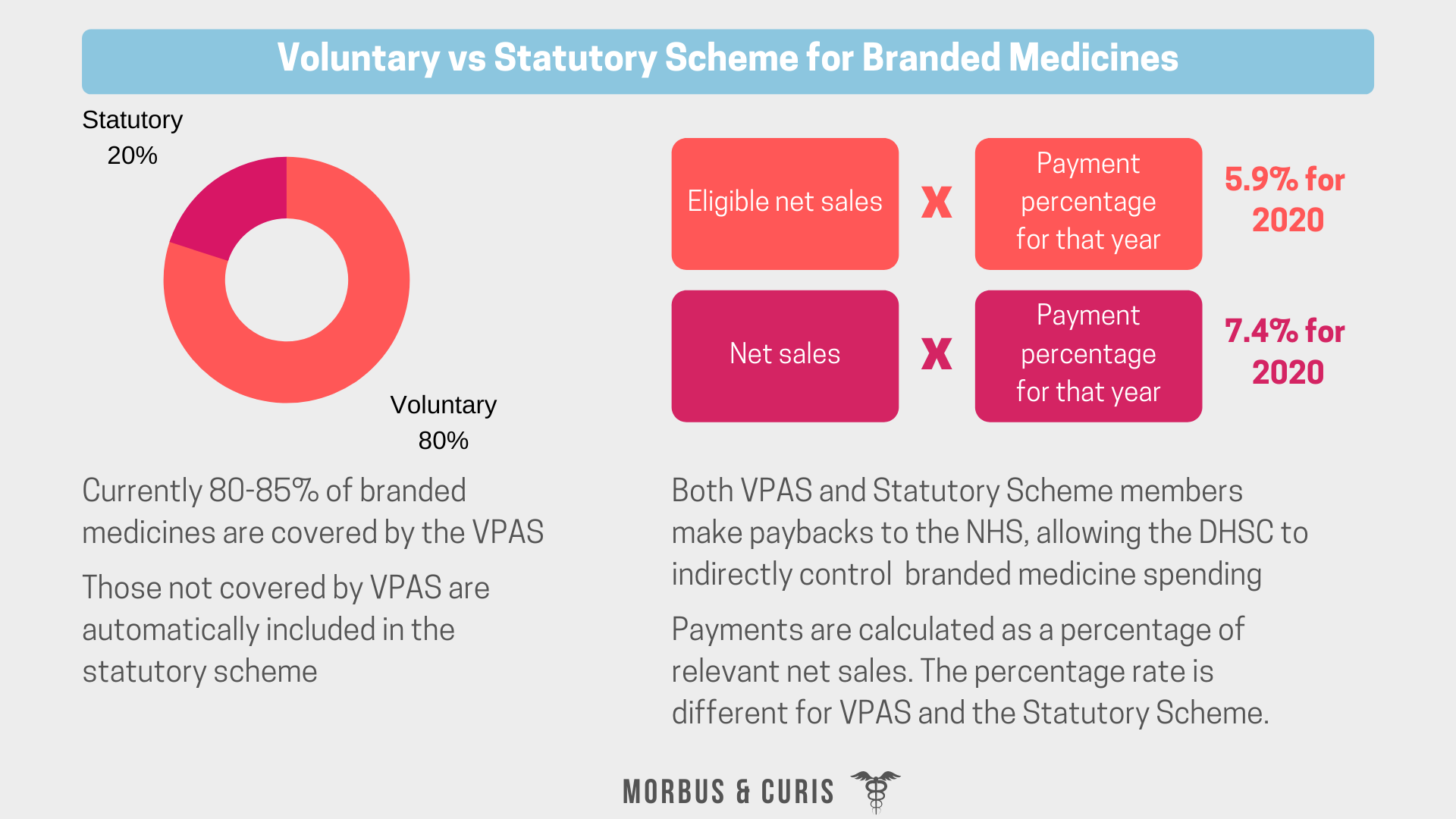
This growth cap is managed via the Voluntary and Statutory Schemes, which both include a payback mechanism. If NHS spending exceeds the agreed percentage growth cap then pharmaceutical companies must pay back a percentage of their net sales to the NHS.
Branded medicines are also assessed by the National Institute of Health and Care Excellence (NICE), who conducts a clinical and cost-effectiveness assessment of medicines via a Technology Appraisal (TA). The outcome of TAs is a recommendation on whether it should be used by the NHS. If NICE decides that a medicine is not cost-effective this can often lead to discussions and negotiations on pricing. The outcome of a NICE assessment is crucial because if NICE does not recommend a product to the NHS and the NHS does not use it, then market share will be very low.
Voluntary Pricing and Access Scheme for Branded Medicines
The Voluntary Pricing and Access Scheme for Branded Medicines is an agreement between the Department of Health and Social Care (DHSC) and the Association of the British Pharmaceutical Industry (ABPI).
It applies to branded medicines, both on and off-patent, that are produced by pharmaceutical companies that have signed up to the scheme. Currently, approximately 80-85% of branded medicines are covered by VPAS, and those not covered by VPAS are automatically included in the Statutory Scheme.

In addition to the growth cap on NHS spending on branded medicines, the scheme contains provisions for the government to control branded medicine prices in various circumstances.
The VPAS provisions include:
A sales growth cap with a payback on NHS overspend
A profit cap
A requirement for the same net price to be offered to all four nations of the UK
Sales Growth Cap and Payback on NHS Overspend
VPAS includes a cap of 2% on the total net sales growth for branded medicines.
If during any year of the scheme, the rise in drug spending by the NHS is above this 2% cap, then scheme members are required to pay back the NHS the overspend.
The payment required from each scheme member is calculated as a percentage of their net sales of relevant medicines. This ensures that their actual branded medicines sales growth is in line with allowed growth.
Profit Cap
VPAS members are subject to an overall profit cap of 6% return on sales and 21% return on capital.
Four Nations, One Deal
VPAS requires that pharmaceutical companies offer the same deal, or rather net price, to all four nations in the United Kingdom.
This could result in industry having to give bigger discounts since any deal agreed with England, the nation with the biggest buying power, would also have to be granted to all of the devolved nations.
However, it could also facilitate faster access since once a deal is negotiated with England, it will automatically be applied across the other nations, thereby saving time.
VPAS and New Active Pharmaceutical Ingredients
In general, manufacturers may set the list price for innovative medicines containing new Active Pharmaceutical Ingredients (APIs). However, VPAS permits the government to have some control over the pricing of innovative medicines containing a new API via the Budget Impact Test. Additionally, it may also influence pricing via its requirement for medicines with new APIs to undergo a technology appraisal by NICE, whose cost-effectiveness thresholds remain unchanged at £20,000 to £30,000 per Quality-Adjusted Life Year (QALY).
Key aspects of the VPAS that apply to innovative medicines containing new APIs include:
Exemption from NHS overspend payback payments
A Budget Impact Test
Prompt NICE Technology Appraisals
Exemption from Payments
Sales of innovative medicines containing a new API are excluded from a pharmaceutical company’s payback payments for their first three years on the market. This aims to promote and incentivise innovation, while the Budget Impact Test provides a financial safety net for the DHSC.
Budget Impact Test
The Budget Impact Test permits the government to have some control over the NHS spend on new APIs manufactured and marketed by VPAS scheme members. This is important for budget stability and predictability since the sales of innovative medicines containing new APIs are exempt from VPAS payback payments.
VPAS requires that if an innovative medicine’s forecast sales are anticipated to exceed £20 million in any of its first 3 years on the market, the pharmaceutical company must alert the DHSC.
Subsequently, NHS England will negotiate list pricing with the manufacturer to avoid this £20 million threshold being exceeded.

More and Faster NICE Technology Appraisals
New legislation requires that all innovative medicines are routinely appraised by NICE. The outcome of a NICE Technology Appraisal is whether it should be recommended to the NHS on the basis of its clinical and cost-effectiveness.
NICE evaluates the cost-effectiveness of a new medicine by comparing the cost per Quality-Adjusted Life Year (QALY) between the innovative medicine and the current standards of care. If NICE decides a product is not cost-effective, this can lead to further price negotiations between NHS England and the pharmaceutical company. The outcome of such negotiations may be a confidential deal that permits the NHS to pay a lower net price for the medicine but ensures access to the majority of the UK market.
The requirement for more and faster NICE appraisals should ensure prompt patient access to medicines that are deemed to be clinically and cost-effective.
Summary of VPAS

Statutory Scheme for Branded Medicines
The Statutory Scheme for branded medicines applies to all branded medicine sales from pharmaceutical companies that have not signed up to the Voluntary Scheme.
It is, in essence, a safety net that allows the government some degree of control over medicine sales growth where companies choose to not become members of the Voluntary Scheme. Similar to the VPAS, it involves a payment of a fixed percentage of sales income from relevant medicines back to the NHS. The percentage rates are slightly higher than the VPAS and less financially attractive for companies whose portfolios contain multiple new APIs. This is because the 3-year exemption on payments for innovative medicines containing new APIs is only available in the VPAS.
Comparison of the Voluntary and Statutory Schemes
Generics
Generic medicines are freely priced and, until recently, were not subject to any direct price controls. Instead, the government relied upon market competition to drive selling and reimbursement prices down.
Normally this system is effective at driving down prices and, on average, generic selling prices are 70–90% lower than the originator within four years of the branded product losing its patent protection.
However, there were several instances where there was a lack of market competition for a specific medicine and generic prices increased dramatically. This was permissible because of a loophole in legislation that prevented the government from controlling the prices of unbranded generics manufactured and supplied by pharmaceutical companies that were members of the voluntary PPRS.
To prevent situations like this reoccurring new legislation was passed in the Health Service Medical Supplies (Costs) Act of 2017, which extended the government’s powers to regulate generic pricing. Now the government can control the price of unbranded generics if it deems an unreasonable or excessive price is being charged. This new price control should prevent any further dramatic price increases for unbranded generics.
Now significant generic price increases need to be approved by the DHSC. Instances where the DHSC may approve a price increase, will likely be limited to those where evidence can be provided to demonstrate that it is no longer economical to supply the medicine or where discontinuation of the medicine would negatively impact patient health outcomes.
The reimbursement price paid by the NHS for generics is determined on a monthly basis with reference to market prices, then published in the Drug Tariff.
Most generics are priced below the reimbursement price or there is a financial disincentive to dispense them. This is because pharmacy and wholesaler margins must also be covered by the reimbursement price.


Unbranded generics are not covered by VPAS or the Statutory Scheme, therefore their net sales are excluded from payback payment calculations.
Procurement Negotiations
Often the list price is not the actual price paid for a medicine. During procurement, NHS England and NHS buying groups can negotiate discounts resulting in the NHS paying a lower net price for a medicine. This is possible in part because of the NHS’s centralised buying power and market share relative to the UK private healthcare market.
Summary
There are multiple factors affecting the prices of medicines in the UK today. From the VPAS and Statutory scheme placing growth caps on total NHS branded medicine spending, to NICE cost-effectiveness assessments and NHS England Budget Impact Tests.

Sources
The Statutory Scheme
The Drug Tariff
If you found this blog post helpful why not consider subscribing.