

T Cell Based Cancer Immunotherapy

Welcome to Morbus & Curis, a blog about disease and healthcare. Today’s blog post is about T cell based cancer immunotherapy (also known as T cell therapy).
We rely on our immune systems to identify and destroy disease-causing pathogens, such as bacteria and viruses. However, not all disease is caused by pathogens. For example, cancer is caused by mutated versions of our own cells that multiply in an uncontrolled way.
Immunotherapy is a type of cancer treatment that harnesses the capabilities of our own immune system to fight cancer. It does so by genetically engineering certain cells in our immune system to better recognise the cancer-causing cell or cell type, so they can be destroyed more efficiently.
To understand how immunotherapy works, it’s important to understand how the immune system works. So, before diving into the details of immunotherapy, here are a couple of brief overviews.
Brief Overview: our Immune System
Our immune system consists of various organs, tissues, cells and processes that help our body fight disease and infection. Our white blood cells are a key player and certain types of white blood cells, known as lymphocytes (or more specifically T and B cells), are the immune systems’ memory. They recognise then help destroy pathogens that the body has previously fought, thereby stopping them from multiplying and causing disease.

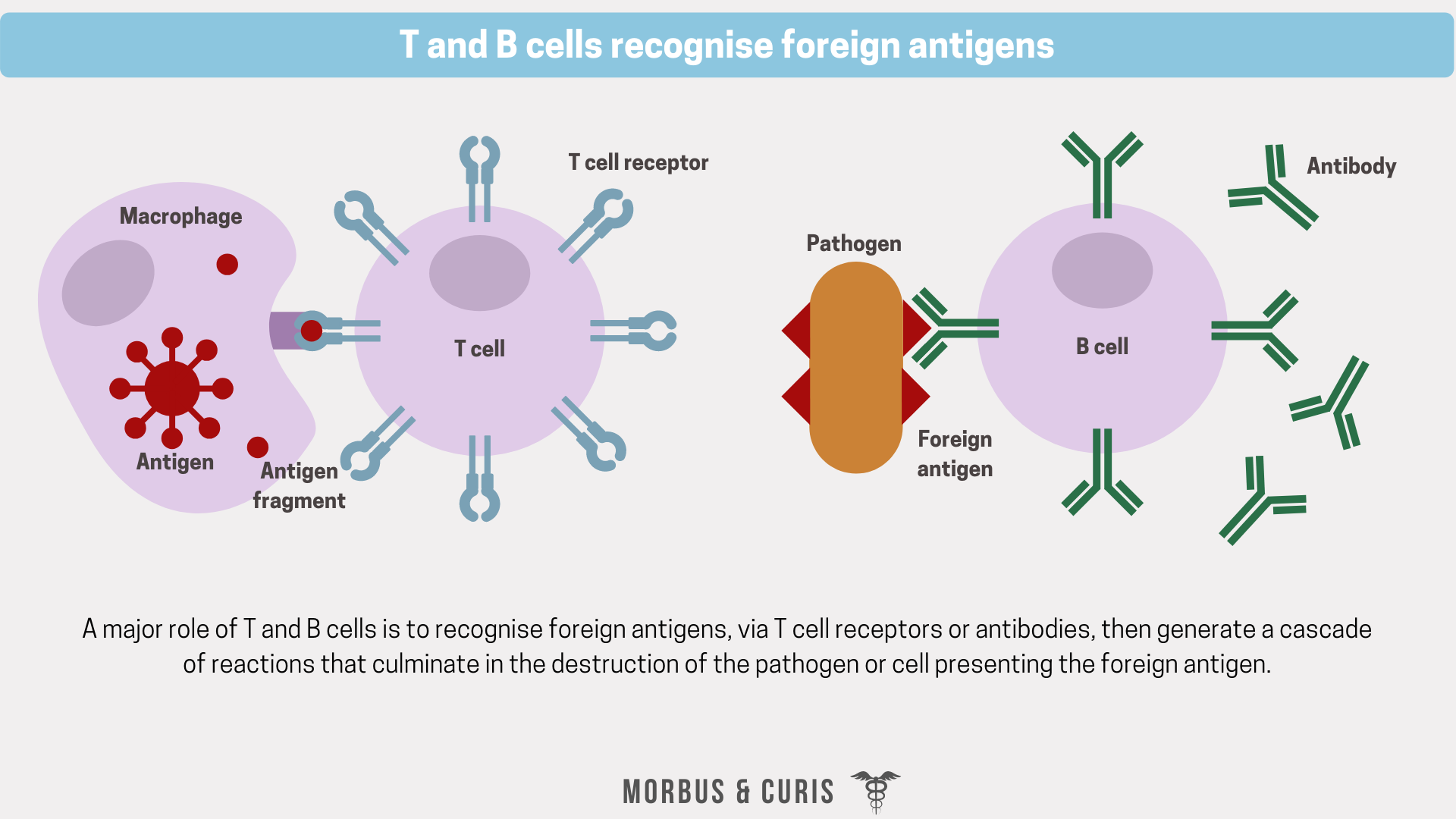
Pathogens are identified by T cell receptors or B cell antibodies, which bind to antigens belonging to the pathogen with high specificity and high affinity. Antigens are like identification tags, which give information about a cell type or what’s inside a cell. They are most often proteins that are displayed on the surface of a cell.
There are two main types of antigen; foreign antigens (those belonging to pathogens, such as bacteria and viruses) and autoantigens (those belonging to your own cells, e.g. proteins exposed on the surface of a healthy cell). Normally, in healthy individuals, T or B cells can specifically recognise foreign antigens via their T cell receptors or antibodies, whose structure complements that of the antigen. The binding site of a receptor or antibody is highly specific, therefore different cell receptors and antibodies recognise and bind to different antigens. There is no master key.
When T cell receptors bind to a foreign antigen and initiate an immune response it’s known as cell-mediated immunity. When antibodies initiate an immune response it’s known as humoral, antibody driven immunity.
Brief Overview: the Immune Response
Once a receptor-antigen or antibody-antigen complex is formed, lymphocytes mediate the destruction of a foreign antigen displaying cell. Here are the different ways in which they orchestrate the destruction of antigen-presenting cells:
B cells mass-produce antibodies that specifically bind to foreign antigens. Antibody binding can:
Trap pathogens in large clumps, in which they are more easily “eaten” by macrophages (macrophages are white blood cells that have a key role in eliminating diseased and damaged cells through their programmed cell death).
Stop viruses from entering other cells, thereby preventing them from multiplying further.
Activated T cells mature into cytotoxic T cells or helper T cells (see illustration below):
Cytotoxic T cells produce cytotoxins, which enter the infected cell or pathogen and destroy it.
T helper cells produce chemicals called “cytokines”, which function as chemical messages that orchestrate the immune response by giving instructions to other immune cells (e.g. they direct B cells to multiply).
Natural killer cells are activated by cytokines and kill infected cells, which they recognise via a change to a surface protein complex called MHC I.

Brief Overview: Cancer
Cancers occur when a genetic change happens in a cell, which results in it dividing in an uncontrolled way. This growth leads to the formation of a tumour, which may later spread elsewhere in the body.
There are many different types of cancers, but they are often categorised according to the cell type they originate from:
Carcinomas (skin cells or cells in tissues lining our internal organs)
Brain tumours (cells in the brain or spinal cord that function in the central nervous system)
Sarcomas (cells in connective or supportive tissue such as bone or cartilage)
Lymphomas (cells of the lymphatic system)
Leukaemias (bone marrow cells responsible for producing white blood cells)
All cells display antigens on their cell surface, including cancer cells. While some antigens are specific to the cell type, others are specific to the cancerous cells.
T Cell Based Cancer Immunotherapy
In T cell immunotherapy a patient’s immune system’s ability to identify and subsequently destroy cancer cells is improved.
There are currently two main types of genetically engineered T cell immunotherapies:
T cell receptor (TCR) T cell therapy
Chimeric antigen receptor (CAR) T cell therapy
Both types of T cell immunotherapy involve genetically engineering T cells so they can recognise an antigen displayed on a tumour cell and bind to it with high affinity. After binding and activation of the T cell, an immune response is initiated resulting in the destruction of that cells presenting that antigen.
The overall process of how these immunotherapy technologies work is similar:
In the first step, a blood sample is taken from the patient. Their T cells are then isolated from the sample.
Next, the T cells are genetically engineered, normally using a disarmed viral vector, to recognise a specific antigen displayed on a tumour cell. The genetic engineering step is where the main differences between TCR and CAR T cell therapy exist.
The genetically engineered T cells are then grown over a few weeks so that there are billions of them.
The patient receives chemotherapy to reduce the number of lymphocytes circulating in their bloodstream. This step effectively makes room for the new modified T cells.
After chemotherapy, the CAR T cells or TCR T cells are infused back into the patient’s bloodstream.
If treatment is successful, the T cells will multiply further and destroy any cancer cells displaying the antigen they’ve been modified to recognise.

The ability of the modified T cells to multiply allows them to remain in the patient and continue to be active for a long time period, essentially giving the patient’s immune system memory against the tumour antigen. This long term immunity gives immunotherapy the potential to be a one-time treatment.
TCR-T Cell Therapy
TCR-T cell therapy involves genetically engineering a patient’s T cells to express an artificially designed T cell receptor that specifically targets a tumour antigen with high affinity.
T cell receptors consist of two polypeptide chains that recognise specific polypeptide antigens that are presented by major histocompatibility complex (MHC) cell surface proteins.
There are pros and cons to T cell receptors only being able to recognise antigens presented by MHC proteins:
One advantage is that MHC proteins can present intracellular antigens, which widens the range of possible targets for TCR-T cell therapy.
One disadvantage is that the T cell receptor is limited to only the antigens presented by MHC proteins and T cell receptor activation is dependent on MHC proteins.

CAR-T Cell Therapy
CAR-T cell therapy involves genetically engineering a patient’s T cells to express a chimeric antigen receptor. This receptor consists of two main parts:
Antigen recognition domain
Signalling domains
The antigen recognition domain is the extracellular part of the receptor. It consists of a single-chain variable antibody domain that recognises and binds to a specific tumour antigen. This domain does not interact with MHC proteins and therefore it cannot recognise and bind to intracellular antigens.
The signalling domains are the intracellular part of the chimeric antigen receptor. They contain the CD3ζ chain of the TCR and costimulatory domains, and function to activate the T cell.

T Cell Therapy Side Effects
T cell therapies clinical trials exposed several potentially lethal side effects associated with these therapies. The two most challenging complications that may occur include:
Cytokine release syndrome (CRS), which results from the huge amount of cytokines being released and it can cause side effects such as high fever, elevated heart rate, reduced blood pressure and breathing difficulties. The symptoms of CRS are mild in some patients but can be life-threatening.
CAR T-related encephalopathy syndrome (CRES), which can lead to headaches, confusion, speaking difficulties, seizures or swelling of the brain (i.e. cerebral oedema, which can be fatal).
However, most T cell therapy side effects are temporary, subsiding within days or weeks of the modified T cell infusion.
In addition to the side effects caused by the T cell transfusion, patients may experience low white blood cell count (neutropenia) and low red blood cell count (anaemia) after chemotherapy. Chemotherapy treatment also has other side effects including fatigue, fever, nausea, vomiting, diarrhoea, hair loss and loss of appetite.
Due to the serious side effects and risks that may be experienced during T cell therapy, approved T cell immunotherapies are not available in all hospitals. Instead, they are administered only in specific hospitals or medical centres where the health care professionals have received extensive training about the treatment. Sometimes these hospitals were also involved in the therapy’s phase III clinical trial and therefore already have experience with the treatment.
Approved Immunotherapies
Currently, only two T cell therapies have been approved by the EMA, and both are CAR-T cell therapies indicated for the treatment of haematological malignancies. There are currently no EMA approved TCR-T cell therapies.
You can find further details about ongoing or completed clinical trials involving T cell therapies for the treatment of cancers here.

Clinical Efficacy of Approved T Cell Therapies
Kymriah
In the ELIANA trial (a single-arm, open-label, multicentre, phase II study to determine the efficacy and safety of Kymriah in paediatric and young adult patients with B-cell ALL who were primary refractory, chemorefractory, relapsed after, or were not eligible for allogeneic SCT), the overall remission rate (ORR) at 3 months was 82%.
In the JULIET trial (an open-label, multicentre, single-arm trial phase II study to determine the efficacy and safety of Kymriah in adult patients with relapsed/refractory DLBCL who received 2 or more lines of chemotherapy), the ORR at 3 months was 50%.
Yescarta
In the ZUMA-1 trial (a phase 1/2 open-label, multicentre, single-arm study in patients with relapsed or refractory aggressive B-cell NHL), the overall remission rate (ORR) at 2 years was 83%.
Future
As new treatments, there is still limited experience with T cell based cancer immunotherapies and still much to learn about them. However, promising initial results mean that over time they could become treatment options for more cancer patients as research in this field of science is increasing and progressing rapidly. Whether they will prove to be effective treatments against solid tumours and whether their safety profile can be improved needs further investigation.
The pricing of T cell therapies may create patient access barriers in some markets where payers do not consider them to be cost-effective against other treatment options or there is a lack of willingness to pay.
For example, Kymriah, which has a list price of £282,000 in the UK, was initially deemed by the National Institute of Health and Care Excellence (NICE) to not be cost-effective for routine funding or use within the Cancer Drugs Fund (CDF). Additionally, there was a lack of data comparing it to salvage chemotherapy, which made it difficult to determine its clinical benefits relative to other treatment options.
After further discussions, the manufacturer agreed to offer Kymriah at a confidential discounted price as part of a managed access agreement. It’s estimated that 200 people (whose disease has not responded or those whose disease has relapsed after treatment with two or more courses of chemotherapy) will now be eligible for treatment with Kymriah each year.
Recommending another revolutionary CAR T-cell therapy for adults with lymphoma represents a step forward for personalised medicine. We are pleased that patients are set to benefit from such an innovative therapy so rapidly because of joint working between NICE, NHS England and the company.
CAR T-cell therapy is expensive, however the treatment is specific to each individual and could be a potential cure for some, although it is early days. Our recommendation for tisagenlecleucel on the Cancer Drugs Fund means people can benefit while more data is collected.
Meindert Boysen, director of the Centre for Health Technology Evaluation at NICE
Sources
First two CAR-T cell medicines recommended for approval in the European Union
NICE encourages further discussions on Kymriah for adult lymphoma
NICE recommends another revolutionary CAR T-cell therapy for adults with lymphoma
If you found this blog post helpful why not consider subscribing.
Cover photo credit: National Cancer Institute on Unsplash