



The Role of Fat in the development of Insulin Resistance

Welcome to Morbus & Curis, a blog about disease and healthcare. Today’s blog post is about the role of fat in the development of insulin resistance.

Insulin resistance is defined as an inadequate response to circulating insulin, and the consequences of insulin resistance vary by organ. For example, in skeletal muscle, insulin resistance can reduce both the rate of glucose uptake and glycogen synthesis. In the liver, it limits the inhibition of gluconeogenesis (glucose production) yet other hepatic pathways, such as lipogenesis (lipid production), are unaffected.
Once insulin resistance is established, type 2 diabetes may develop. This occurs when pancreatic beta cells can no longer produce enough insulin to compensate for increased insulin resistance and blood glucose levels start to rise.
The causes of insulin resistance remain a popular area of research as the worldwide prevalence of type 2 diabetes continues to soar. One area that seems to be getting more interest is the role of fat in the development of insulin resistance.
To better understand how fat can influence an individual’s risk of developing insulin resistance, let’s look at how it can affect various organs.
The Effects of Fat in the Hypothalamus
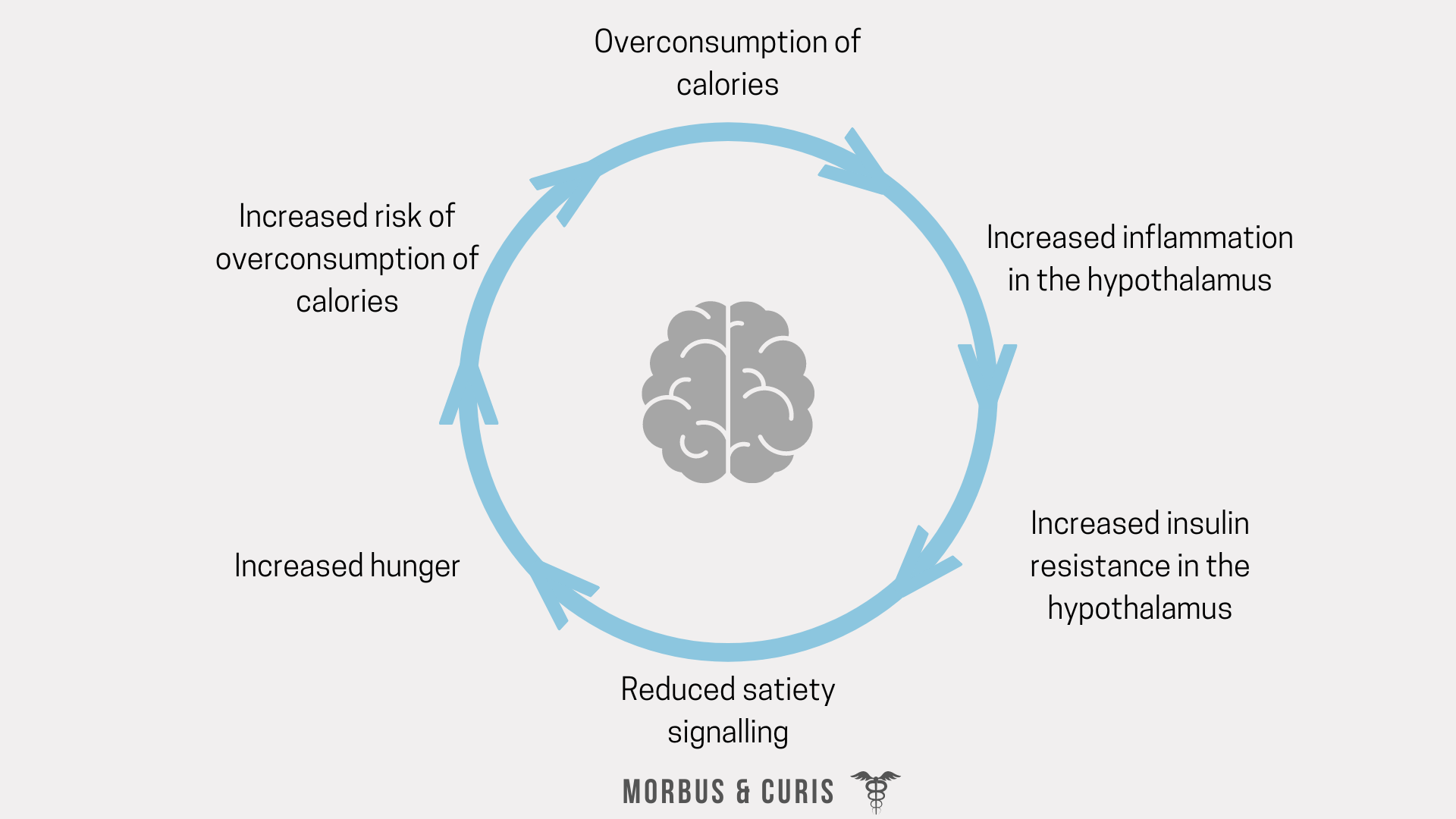
The role of the hypothalamus is to match energy intake with energy expenditure. If the hypothalamus fails in this role it can lead to overconsumption of calories and the excess calories are stored as fat.
However, there’s a bit of a vicious cycle at play. Consuming excess calories or a high amount of saturated fat has been shown to increase inflammation in the hypothalamus. This, in turn, reduces hypothalamic sensitivity to insulin and leptin satiety signalling, attenuating satiety and increasing hunger. This then increases the risk of overconsumption of calories.
After consumption of a meal containing high levels of fat, free fatty acid levels circulating in the bloodstream rise and are sensed by the hypothalamus. However, the hypothalamus responds differently to different fatty acids and they have varied effects on the function hypothalamus and its insulin sensitivity.
For example, if the hypothalamus senses high concentrations of the saturated fatty acid, palmitic acid, then it releases cortisol, which worsens insulin resistance.
Conversely, if the hypothalamus senses high levels of oleic acid, a monounsaturated omega-9 fatty acid, this acts as a signal of nutrient abundance. In response to high concentrations of oleic acid, the levels of NPY, an appetite-inducing hormone, are reduced resulting in increased satiety. Additionally, it’s also been shown that consumption of omega-3 fatty acids can reduce inflammation and therefore insulin resistance in the hypothalamus.
Thus the type of fat we consume plays a key role in hypothalamic insulin resistance and satiety signalling.
The Effects of Fat in Adipose Tissue
The inflammation caused by caloric excess or overconsumption of saturated fat can also lead to increased insulin resistance in adipose tissue.
Normally fat cells can safely store fat, after all, that is one of their key roles in the body! However, caloric excess or excess saturated fat consumption can lead to over-expansion of fat cells. This causes inflammation, which increases the insulin resistance of the fat cells.
One way the body can avoid the over-expansion of fat cells during a state of caloric excess is to generate new fat cells. New adipose cell generation is mediated by PPAR𝛾, a gene transcription factor that controls the expression of various adipose-specific genes. However, the activity of PPAR𝛾 is negatively regulated by inflammatory cytokines, demonstrating that inflammation can further exacerbate insulin resistance in adipose tissue by preventing the generation of new fat cells.
Conversely, the activity of PPAR𝛾 is increased by omega-3 fatty acids and polyphenols, again highlighting the importance of dietary fat quality.

The Effects of Fat in the Liver
Unlike adipose tissue cells, the cells of the liver are not able to safely store excess fat. When fat accumulates in the liver it’s known as non-alcoholic fatty liver disease and is associated with increased insulin resistance.
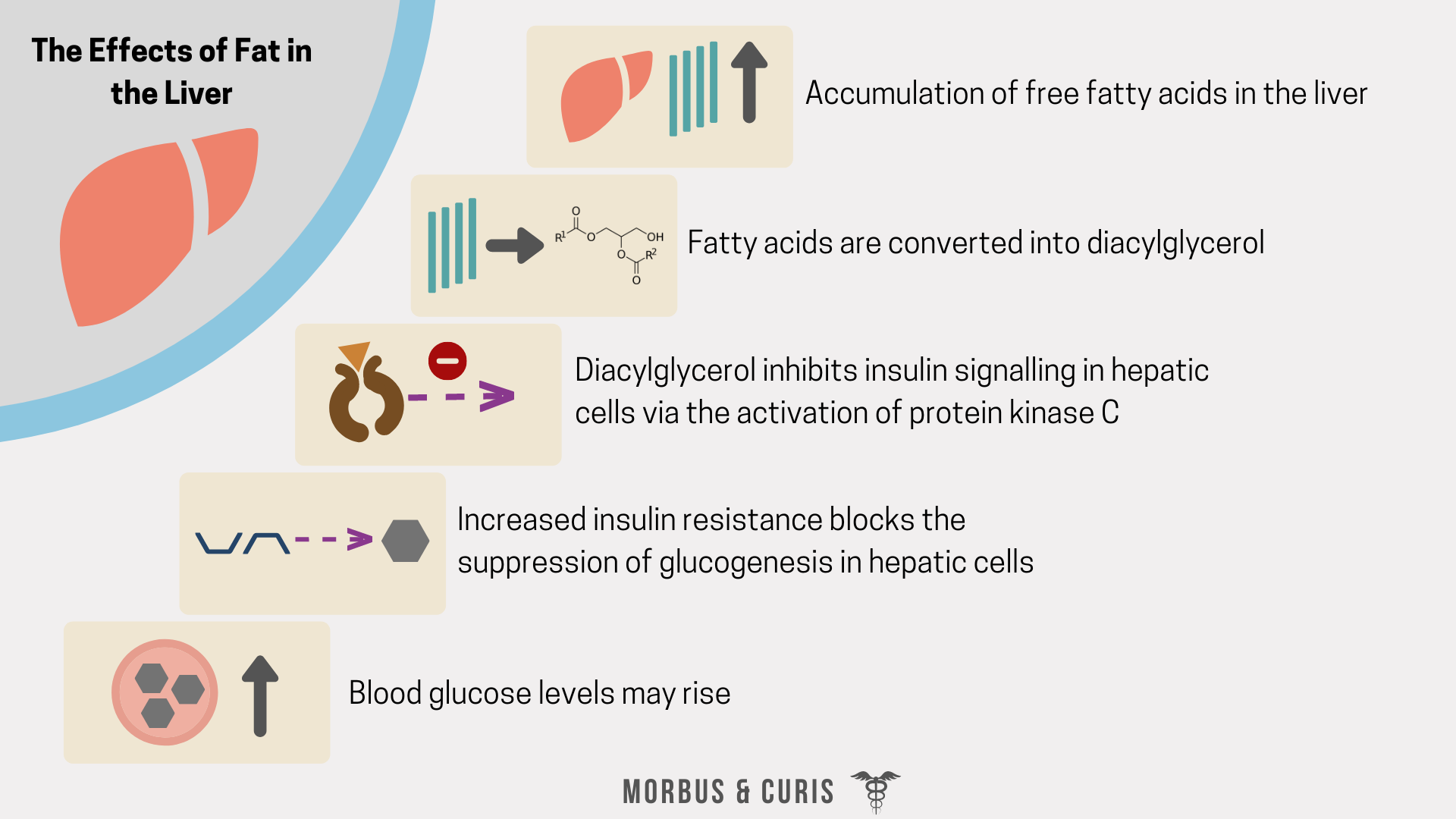
The liver has a central role in lipid metabolism through its ability to convert free fatty acids and glucose into triglycerides, which then enter the circulation as lipoproteins. High levels of circulating free fatty acids can further exacerbate insulin resistance in the liver. This occurs if hepatic cells are not able to convert fatty acids into triglycerides fast enough and some fatty acids are converted into diacylglycerol, which inhibits insulin signalling by the activation of protein kinase C.
The liver also has a key role in glucose homeostasis through its ability to reversibly convert glucose into glycogen. Insulin resistance in the liver blocks the suppression of glucogenesis. Consequently, even when blood glucose levels are high, hepatic cells continue to break down glycogen and release glucose into the circulation, maintaining or worsening high blood glucose levels.
The Effects of Fat in Skeletal Muscle Tissue
The mechanisms underlying free fatty acid-induced skeletal muscle insulin resistance are not fully understood.
Firstly, overconsumption of fat can indirectly influence skeletal muscle insulin resistance by causing systemic inflammation. For example, circulating inflammatory cytokines, such as TNF𝛼, increase insulin resistance in skeletal muscle tissue by disrupting the insulin signalling pathway.
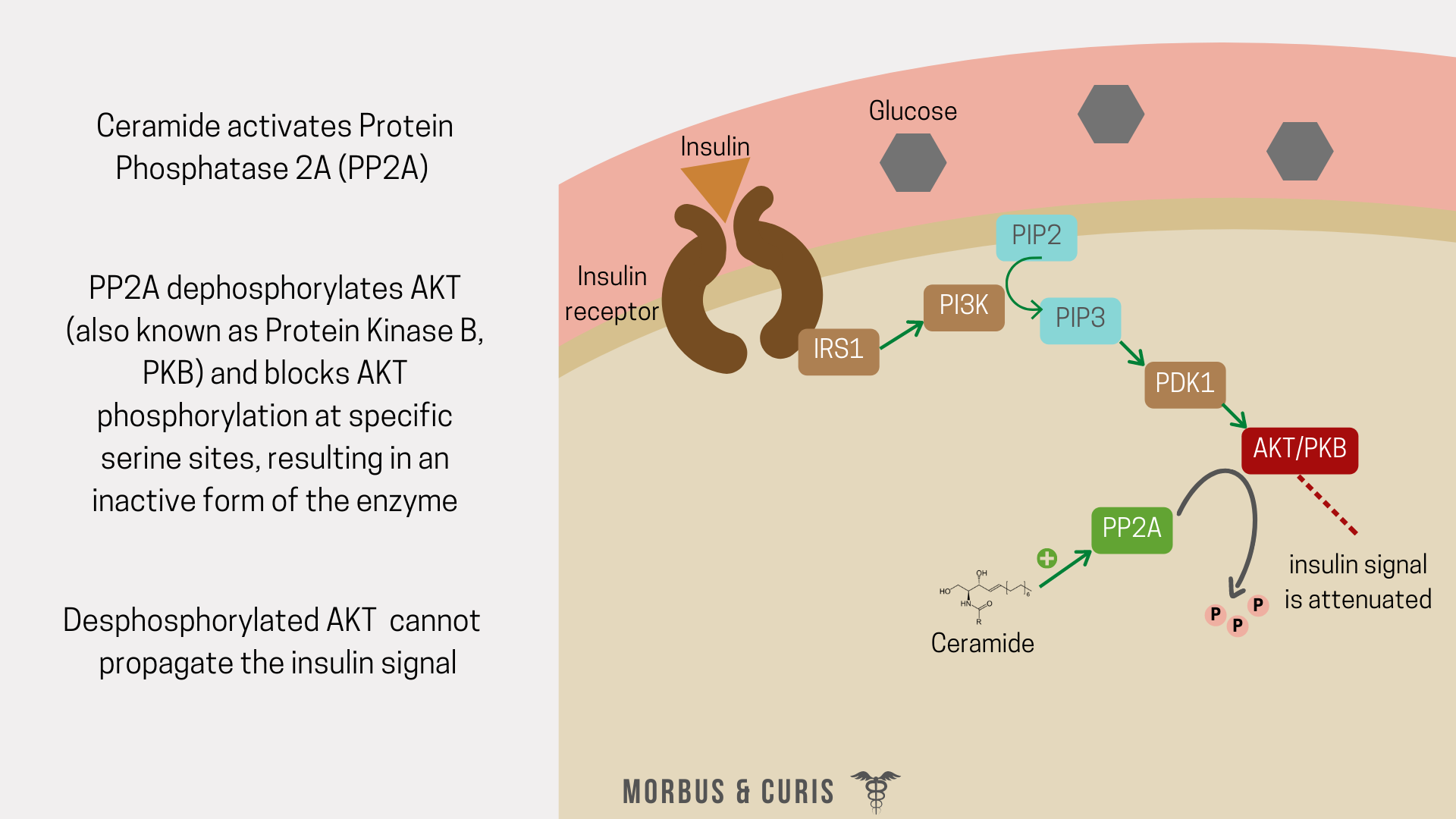
Secondly, the accumulation of saturated fatty acids in skeletal muscle tissue can increase insulin resistance when they bind to the TLR-4 receptor and block the oxidation of fatty acids. This causes fatty acids to accumulate in the cytoplasm and makes palmitic acid available to be converted into ceramide. Ceramide blocks insulin signalling by activating protein phosphatase 2A which inhibits AKT.
The effects of excess lipids can be reversed through exercise, which induces the oxidation of fatty acids that have accumulated in the skeletal muscle cells.
The Effects of Fat in the Pancreas
Pancreatic beta cells are responsible for the production and secretion of insulin. While saturated fatty acids clearly affect insulin resistance in some organs, in the pancreas it appears to affect beta cell function, including insulin production.
When circulating levels of saturated free fatty acids and glucose are high in the presence of pro-inflammatory cytokines, this is believed to create a glucolipotoxic state that damages beta cells through oxidative stress.
Oxidative stress is mediated by lipoxygenases that oxygenate intracellular polyunsaturated fatty acids into inflammatory lipid compounds that negatively impact cellular function and can induce cell death. For example, the lipoxygenase 12-LO, which is activated by a high fat diet, catalyses the production of 12-HETE, a pro-inflammatory compound that has been demonstrated to negatively affect beta cell function and induce beta cell death.
Additionally, the saturated fatty acid, palmitate, has been shown to induce β cell dysfunction in vivo by activating inflammatory processes.
Conversely, monounsaturated oleic acid has been demonstrated to have a protective effect on β cells, leading to improvement in cell proliferation, triglyceride accumulation and insulin secretion.
The Effects of Fat in the Gastrointestinal Tract
The composition of an individual’s diet has a huge influence on the microbial composition of their gastrointestinal tract.
It’s been demonstrated that both obesity and a high fat diet can increase the permeability of the intestines. This allows lipopolysaccharide (LPS), a component of the bacterial cell wall of Gram-negative bacteria, to cross over the epithelium and enter the bloodstream.
Once in the circulation, LPS can bind to LPS binding protein then interact with TLR-4 receptors, inducing an inflammatory response via the activation of pro-inflammatory kinases and the release of TNF𝛼. Circulating TNF𝛼 then increases insulin resistance in a variety of tissues, by impairing IRS-1, Akt and AS160 phosphorylation as well as GLUT4 transporter translocation.

Summary
The total fat intake and the type of fat consumed by an individual has a clear impact on the level of insulin resistance in various organs and beta cell function.
Saturated fat and elevated levels of circulating free fatty acids significantly worsen insulin resistance, while monounsaturated and polyunsaturated fatty acids appear to improve insulin sensitivity in some organs.
Sources
The role of fatty acids in insulin resistance
What causes the insulin resistance underlying obesity?
Beta Cell Dysfunction and Insulin Resistance
12-Lipoxygenase and Islet β-Cell Dysfunction in Diabetes
12-Lipoxygenase Promotes Obesity-Induced Oxidative Stress in Pancreatic Islets
Roles of diacylglycerols and ceramides in hepatic insulin resistance
If you found this blog post helpful why not consider subscribing.
Cover photo credit: Thomas Park on Unsplash